AIMS Journal, 2019, Vol 31, No 4
By Linn Shepherd

Administration of synthetic oxytocin - induction of contractions
Synthetic oxytocin has been used since the 1950s for induction and augmentation of contractions. Induction and augmentation only differ in that induction is to try to start labour, whilst augmentation happens after contractions have started, to improve their strength or organisation, and make them more efficient.
In the UK, ‘Syntocinon’1 is the name that most people associate with synthetic oxytocin, but other companies now produce synthetic oxytocin under the simpler name ‘Oxytocin’.
According to the approved instructions licensed for synthetic oxytocin for induction and augmentation of labour, the concentrate should always be a well-diluted solution for administration intravenously, and never administered undiluted, by intramuscular injection before the baby has been born.
When a woman has consented to intravenous synthetic oxytocin, the infusion (controlled by an electric pump) will be started:
Limitations set by the licensed instructions for synthetic oxytocin
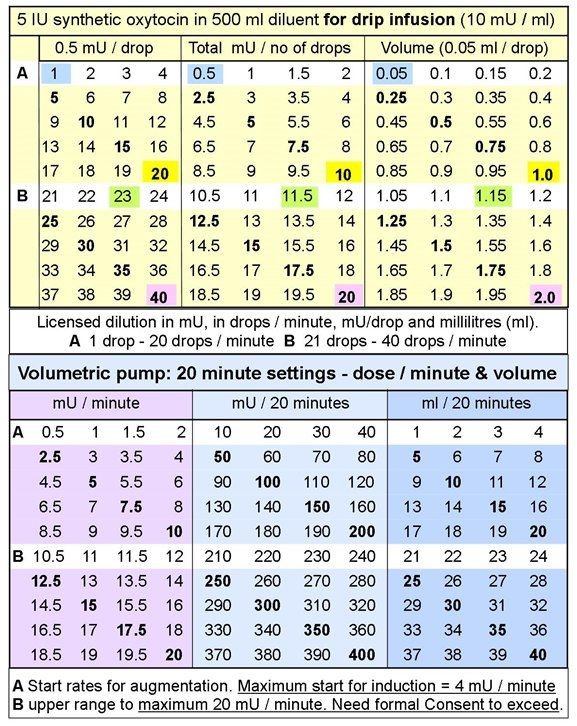
The maximum dose of synthetic oxytocin to start an infusion when no contractions are present is 4 milliunits per minute (4 mU/min).
Increases of infusion rate can be made from 20 minutes after the previous increase, at no more than 2 mU/min more than the previous infusion rate. The licensed terms of use and guidance for managing synthetic oxytocin infusion should be applied in all cases aiming to reduce the rate slightly - if possible - once labour is established, to minimise the input of synthetic oxytocin in the presence of maternal oxytocin.
See Figure 1 below for an illustration of the dosages.
Good practice when using synthetic oxytocin
During augmentation of labour, it may be possible to start with less than 4 mU/min because maternal oxytocin is already at work. If the initial rate-per-minute of the intravenous infusion has not achieved the desired effect (about 3 contractions in 10 minutes), the dosage rate is speeded up slightly.
Fine-tuning with smaller increases of 0.5 mU/min or 1 mU/min can be tried first, to blend with maternal oxytocin.
Standard prescribing practices
If a doctor prescribes you medicine, the prescription relays instructions to the pharmacist, who checks the prescription, and provides the requested drugs clearly labelled with the name of the drug, your name, information about the dose and timings of the doses, and any warnings, such as ‘Do not exceed stated dose’. If a pharmacist is concerned that a mistake has been made with a prescription, they have processes to follow to address this.
Doctors can prescribe drugs that are not licensed for pregnancy for the condition you have and at greater doses than are recommended, if the licensed dose has been ineffective. When prescribing a higher dose, they should explain their reasons during the discussion with you, and formally obtain your consent.
Current prescribing of synthetic oxytocin
Hospital doctors should also follow this standard of prescribing procedure for every use of synthetic oxytocin that does not adhere to the licensed instructions. But somehow synthetic oxytocin,1 as it is currently being prescribed for during and after labour, is slipping through the ‘consent’ net. The RCOG’s recommended regime advises dilutions, dosage steps and a final maximum that all rise well above the recommended and (therefore) licensed limitations and this is not being explained to women, and their consent is not being obtained.
If unlicensed dilutions are declined by women who wish to receive the licensed dilution with full dosage range and fine-tuning options (via volumetric pump), in hospitals where only syringe drivers are available, a drip infusion can be requested, as a midwife will (or should) be in attendance continuously.
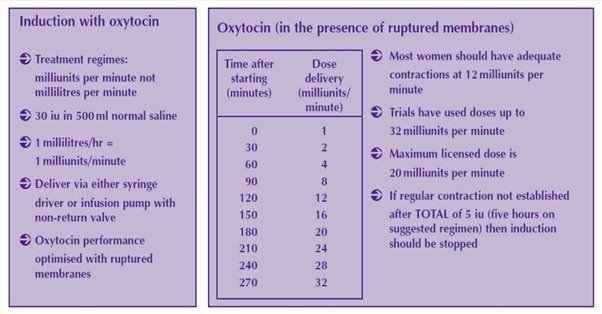
See Figure 2 below, which is from the Royal College of Obstetricians and Gynaecologists, called 'active mangement', first issued in 2001.3, 4
These RCOG guidelines suggest that after rupture of membranes (whether spontaneously or artificially), the infusion should be started at 1 mU/min, being raised to the licensed maximum (20 mU/min) by three hours later. In practice, contractions should start and settle5 in the range from 4–12 mU/min.
The recognition of early disorganised contractions and their attempt to organise themselves is an important skill which midwives should develop to protect patients from receiving an unnecessarily high infusion rate, which risks desensitising oxytocin receptors, thus causing contractions to ease off. The midwife may mistakenly assume that a higher infusion rate is needed, but it would be better to reduce the infusion to the rate when contractions were last palpable, and wait a bit longer.
Always, infusion rates should be increased only according to the clinical need, to improve the contraction rate without losing complete relaxation for at least a minute between them. (The clock times on a table of infusion rates are a loose guide only.)
Consent and additional risk factors
This article highlights the need for doctors and prescribing midwives working in NHS hospitals to restore standard consent procedures to hospital practice for the RCOG’s unlicensed synthetic oxytocin regimes, and to inform women of other choices open to them, such as the licensed dosage range.
The RCOG’s unlicensed synthetic oxytocin regime comes with the National Institute for Health and Care Excellence’s (NICE) recommendation for an epidural in advance, accepted by many women, and the loss of fine-tuning options, which increase the risk of overly-strong contractions, fetal distress, complicated births and postpartum haemorrhage.6
Providing this information, and seeking informed consent for unlicensed regimes, is not only the legal standard that women should expect from doctors registered to practise in the UK, but it protects non-prescribing practising midwives from seeking consent for unlicensed synthetic oxytocin regimes, for which they are not qualified or covered to take responsibility. It also protects prescribing midwives and doctors from potential allegations of assault for treatment carried out without informed consent, therefore finding themselves in conflict with the Montgomery ruling.7
Obtaining valid informed consent cannot be skipped over as too challenging or too time-consuming. The prescriber must have clinical reasons for going ‘off licence’ (as required by the RCOG’s regime); must explain these to the woman; must warn her of the risks being added to her labour in so doing, also describing any benefits offsetting those risks; and must accept the woman’s decision if she declines.
Regardless of what a woman has agreed to earlier in the labour or before labour, a doctor must request consent again following a full assessment of the patient, if they find what they consider to be an obstetric reason to prescribe over 20 mU/min (the licensed maximum). If the woman declines, 20 mU/min must not be exceeded. It is illegal for the doctor to proceed - as implied in many synthetic oxytocin policies - without formal consent.
In all cases, people can change their minds after consenting to any drug or procedure and it must be discontinued. It is illegal to start or continue a procedure or treatment for which consent has not been given, or after consent has been withdrawn.
Practical implications of the RCOG’s regime
The RCOG regime increases the dosage range to 32 mU/min, as shown in Figure 2 below, 12 mU/min over the maximum licensed dose! The inflexibility of this regime, now used all across the UK, means that the optimum infusion rate for as natural a labour as possible may be missed for some women.
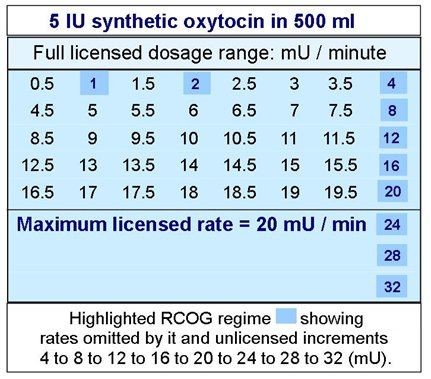
See Figure 3 below for the rates omitted by RCOG, and the unlicensed increments
This regime is administered from a variety of unlicensed dilutions using volumetric pumps (or syringe drivers that offer 50 ml of intravenous solution at a time). For volumetric pumps, synthetic oxytocin is added to 500 ml suitable diluent, but the ability of volumetric pumps to provide an accurate dose is reduced when they are run at the slowest rates, as is required by the unlicensed dilutions recommended by the RCOG, of 10 IU or 30 IU in 500 ml.
The licensed 5 IU in 500 ml facilitates the full dosage range in a greater volume of fluid which can be administered more accurately via volumetric infusion pump.
The unlicensed increments of the RCOG’s regime (after 4 mU/min) reduce the likelihood of successfully fine-tuning the infusion with maternal oxytocin, as only when changes of 0.5 mU/min are available (an option in the licensed instructions) can fine-tuning be achieved. While this situation persists with the RCOG’s regime, so does the likelihood of partially desensitising oxytocin receptors.8
When using syringe drivers to administer the infusion, it has been common for trusts to permit 10 IU in 50 ml (twenty times stronger than the licensed dilution) so that 50 ml lasts longer. The syringe driver is more efficient than a volumetric pump, and fine-tuning is possible (although not being practised) but the bolus option should be disabled before a synthetic oxytocin infusion is started, because 0.5 ml of 200 mU/ml would risk fetal or maternal distress if accidentally infused.
Some trusts use weaker dilutions in their syringes but none uses the licensed dilution.
In other words, the full range of licensed options has not been transferred into the RCOG’s regime. Currently, no in-between rates are supplied for midwives to even try fine-tuning (see Figure 2 below). The clinical effects of not being able to control a synthetic oxytocin infusion optimally, within the recommended dosage range as licensed, include contractions coming too often and/or lasting too long and/or allowing too little relaxation between, such that the biochemistry of normal contractions gets progressively out of sync risking an increase in fetal distress, that may lead to caesarean section in first stage or instrumental delivery at the end of second stage, and also postpartum haemorrhage after third stage. All of which may impact the baby and will certainly impact the mother, both during this birth and in subsequent pregnancies and births.
Importantly, the dilutions being used to facilitate the RCOG’s regime should be deemed pharmacological because they function as a drug, instead of blending with maternal oxytocin physiologically, as the licensed dilution can achieve. Theobald (1965) stated, ‘it has never been shown that the pharmacological drip is more effective than the physiological one, and it is certainly less safe’.9
(A half-strength physiological dilution can also be therapeutically effective.10)
Synthetic oxytocin and other effects on blood pressure
Physiological dilutions of synthetic oxytocin normally reduce blood pressure slightly, but pharmacological dilutions more-so.
When the latter also require epidural for relief of otherwise shock-inducing pain, blood pressure also falls due to the epidural. The natural response to shock is also lowered blood pressure to facilitate oxygenation of distressed tissues.
The overworking of the uterine muscle stimulated to contract by synthetic oxytocin over a period of hours, and sometimes without sufficient time to recover between contractions, produces acidosis which naturally leads to vasodilation - yet another blood-pressure-lowering effect. Acidosis also affects the unborn baby.
If oxytocin receptors are desensitised as well, their part in achieving vascular and muscular tone when it is needed at the end of labour is diminished or removed. Brindsden and Clark (1978) discuss this in their research report on postpartum haemorrhage following their trial with experimentally large increments of synthetic oxytocin.11
These five factors make a major contribution to excessive bleeding after birth, which could be prevented by using so little synthetic oxytocin that maternal oxytocin controls postpartum bleeding in the same way as after a spontaneous labour.
Is a shorter labour actually a benefit?
It is common for the term ‘shorter labour’ to be touted as a benefit of the use of synthetic oxytocin. But, even if the length of labour is actually being reduced on average, are individual women actually benefitting from this? Length of labour for an individual cannot be known beforehand, so determining whether an individual’s labour has or has not been shortened by the ‘active management’ of their labour is not possible. So justifying high doses of synthetic oxytocin for this reason does not make sense.
Do epidurals mean the increased pain of induced labour is not an issue?
Giving an epidural that successfully obliterates the pain generated by higher-than-necessary doses of synthetic oxytocin might address the issue of the pain, but it does not overcome the other potential risks from the use of unlicensed synthetic oxytocin, and an epidural itself introduces new risks.
Care of women during induction of labour
When a woman agrees to prostaglandins treatment, or a synthetic oxytocin infusion, it is important that midwives recognise her status as a patient undergoing treatment, with new care needs which are more complex than the natural biochemical interactions of spontaneous labour.
This is because the synthetic oxytocin infusion requires continuous supervision by a qualified professional, and as many fine adjustments as necessary, according to its effect on the woman, the baby’s tolerance of it, and to ensure every relaxation between contractions lasts for one whole minute or more. Therefore, the woman can never be left on her own with the infusion still running. This is clearly stated in the instructions, and underlined by advice from the World Health Organisation.12
If the midwife has to leave the woman, then the synthetic oxytocin infusion should be paused, and this should be recorded in the notes and on the cardiotocography (CTG) trace. After the midwife returns, she should count the fetal heart with a Pinard’s stethoscope to check that it is still in the normal range and reassess the contractions for 10 minutes. If all other observations are normal (and recorded), the infusion can be restarted at a slightly lower rate than when it was paused. These details must also be recorded in the notes.
Finishing labour after physiological dilutions of synthetic oxytocin
Once labour is established, the infusion can often be slightly reduced. An additional benefit of fine-tuning synthetic oxytocin is that, as far as possible, the rest of labour proceeds under the influence of maternal oxytocin with no further infusion rate increases.
During second stage, as expulsive contractions begin, maternal oxytocin rises significantly,13 allowing for synthetic oxytocin to be stepped down and discontinued within the hour before the baby is born.
When this handover between synthetic oxytocin and physiological labour is conducted with skill during second stage, after third stage (birth of the placenta) natural oxytocin normally achieves a sustained, spontaneous contraction that prevents excessive postpartum bleeding. Traditionally, a midwife stays another whole hour to check regularly that the womb is well-contracted, or bleeding is well-managed.
Restoring choice to clinicians and women
Nearly-natural labours are well within reach when the synthetic oxytocin infusion is managed according to the licensed instructions. Reinstating them formally is an essential consideration for Trusts, both from a safety and a legal perspective, as the standard licensed dilution is strong enough for its role to enhance sluggish contractions, without desensitising oxytocin receptors.
Remembering the baby
The baby should not be accepted as ‘the canary in the mine’ to indicate when something is wrong, rather than eliminating predictable causes of fetal distress beforehand.14 The ability to fine-tune synthetic oxytocin during labour is the most accessible way to prevent fetal distress during induced and augmented labour, or to address it immediately by slowing or discontinuing the infusion. It should be noted that fetal distress can occur for other reasons when synthetic oxytocin is not in use, which is why fetal distress when sythetic oxytocin is in use, must immediately be taken seriously.
Summary
Consent from the woman for synthetic oxytocin infusion must always be sought, but currently no-one is informing women that when synthetic oxytocin is recommended, it is likely to be prescribed and administered in unlicensed dilutions and increments, with regular disregard for the benefits and safety measures built into the licensed instructions.
Restoring fully informed consent procedures, and the licensed dosage range as a valid option to be selected by women, doctors and midwives for a myriad of clinical reasons - and a natural maternal desire for as normal an outcome of labour as possible - promotes far better outcomes for women and babies, and higher professional satisfaction.
Illustrative tables
The following tables may be useful to give to your midwife or doctor to illustrate the figures and calculations in this article. In the Key and charts, 1 International Unit (IU) = 1000 milliunits (mU).
|
|
|
|
|
Figure 3 - Full Licensed Dosage Options Modified and Extended by the RCOG (2001,2008) |
|
|
|---|
|
|
Linn Shepherd is a retired nurse-midwife from Scotland, who practised midwifery in Scotland and England until leaving to raise her children. She has investigated the early research that underpins the instructions licensed for intravenous infusions of synthetic oxytocin, for outcomes of enhanced obstetric labour comparable to those of spontaneous labour.
References
1. Mylan Ltd has taken Syntocinon® over from Novartis, who had the licence from 1977 to 2018. Other UK manufacturers call their product ‘Oxytocin’. https://www.medicines.org.uk/emc/product/9457/smpc
2. STEER PJ, LITTLE DJ, LEWIS NL et al. (1975). ‘Uterine Activity in Induced Labour’. BJOG: An International Journal for Obstetrics and Gynaecology 82(6): 433-441. http://onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.1975.tb00666.x/full
3. ROYAL COLLEGE OF OBSTETRICIANS AND GYNAECOLOGISTS: Setting Standards to Improve Women’s Health (2001). ‘Induction of Labour: Evidence-based Clinical Guideline Number 9’. Page 13 (24 of 90). http://www.perinatal.sld.cu/docs/guiasclinicas/inductionoflabour.pdf
4. NATIONAL COLLABORATING CENTRE FOR WOMEN’S AND CHILDREN’S HEALTH (UK): Funded to Produce Guidelines for the NHS by NICE (2008). ‘Induction of Labour, 2nd Edition’. Clinical Guideline 2008, No. 70. Section 2:88 (106 of 124), Appendix D, Table D.2, footnote b. Published by RCOG Press. https://www.nice.org.uk/guidance/cg70/evidence/full-guideline-pdf-241871149
5. BEAZLEY JM, BANOVIC I and FELD MS (1975). ‘Maintenance of Labour’. British Medical Journal 2(5965): 248-250. https://www.bmj.com/content/bmj/2/5965/248.full.pdf
https://doi.org/10.1136/bmj.2.5965.248
6. BUDDEN A, CHEN LJY and HENRY A (2014). ‘High-dose versus Low-dose Oxytocin Infusion Regimens for Induction of Labour at Term’. Cochrane Database of Systematic Reviews. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD009701.pub2/full
7. BRAMLEY S (2019). ‘Consent to Treatment Post Montgomery - plus ça change?’. AIMS Journal 31(3). https://www.aims.org.uk/journal/item/montgomery
8. VRACHNIS N, MALAMAS FM, SIFAKIS S et al. (2011). ‘The Oxytocin-Oxytocin Receptor System and Its Antagonists as Tocolytic Agents’. International Journal of Endocrinology 2011:350546. Open Access online at https://www.hindawi.com/journals/ije/2011/350546/ http://dx.doi.org/10.1155/2011/350546
9. THEOBALD GW (1965). Letter, ‘Buccal Oxytocin’. British Medical Journal 1(5428): 190-191. https://www.bmj.com/content/1/5428/190.5
10. MANSY A (2017). ‘Does Labor Augmentation with Oxytocin Increase the Risk of Postpartum Hemorrhage? A Randomized Controlled Trial’. Clinics in Mother and Child Health 14:3 https://www.longdom.org/open-access/does-labor-augmentation-with-oxytocin-increase-the-risk-of-postpartumhemorrhage-a-randomized-controlled-trial-2090-7214-1000268.pdf
11. BRINSDEN PRS and CLARK AD (1978). ‘Postpartum Haemorrhage after Induced and Spontaneous Labour’. British Medical Journal 2(6141): 855-856. https://www.bmj.com/content/bmj/2/6141/855.full.pdf
12. WORLD HEALTH ORGANIZATION (2017). Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors, 2nd edition. P-23: 355 of 492 . Free PDF download (4.26 MB) at http://www.who.int/maternal_child_adolescent/documents/managing-complications-pregnancy-childbirth/en/ ISBN: 978-92-4-156549-3
13. BERDE, B. (1965) ‘Some Observations on the Circulatory Effects of Oxytocin, Vasopressin and Similar Polypeptides’. P 11 and 'Release of Oxytocin during Parturition'. P 51. Advances in Oxytocin Research: Proceedings of a Symposium held by the Blair-Bell Research Society at the RCOG on the 1st May. (ed) J, H, M, Pinkerton. London. Pergammon Press Ltd. eBook ISBN: 9781483156507
14. WEEKS A and NEILSON J (2015). ‘Rethinking Our Approach to Postpartum Haemorrhage and Uterotonics’. British Medical Journal 2015;351:h3251. https://doi.org/10.1136/bmj.h3251
https://livrepository.liverpool.ac.uk/2047825/1/Weeks%20Neilson%20BMJ%202015%20351%20h3251.pdf
[Dosage tables courtesy of www.oxytocinmeasures.com. Other info is at: GMC website, NMC website, Birthrights.org.uk]
The AIMS Journal spearheads discussions about change and development in the maternity services.
AIMS Journal articles on the website go back to 1960, offering an important historical record of maternity issues over the past 60 years. Please check the date of the article because the situation that it discusses may have changed since it was published. We are also very aware that the language used in many articles may not be the language that AIMS would use today.
To contact the editors, please email: journal@aims.org.uk
We make the AIMS Journal freely available so that as many people as possible can benefit from the articles. If you found this article interesting please consider supporting us by becoming an AIMS member or making a donation. We are a small charity that accepts no commercial sponsorship, in order to preserve our reputation for providing impartial, evidence-based information.
AIMS supports all maternity service users to navigate the system as it exists, and campaigns for a system which truly meets the needs of all.