AIMS Journal, 2025, Vol 37, No 2

By Nicole Schlögel
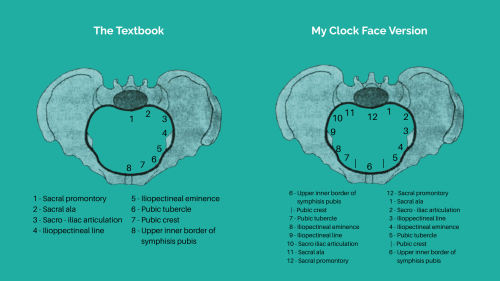
“Iliopectineal line, iliopectineal eminence, pubic…”.
We are halfway through the eight landmarks of the pelvic brim, a choir of student midwives reciting their psalms. We are practicing for our anatomy of childbirth exam by reading the words off the screen at the front of the classroom. I am grateful that I have a basic grasp of anatomy thanks to my training in body massage and aromatherapy and I am curious to learn where the connections lie between my grounding in holistic health and the art of midwifery. It is 2006, I am almost through my first year of midwifery school.
Tiny particles of dust dance in the beam of light that forms the image our lecturer, Sharon, is pointing at, and as I watch them, I set my intention: ace this part of the exam. It seems easy enough to commit to memory the eight names I have been reading out in unison with my peers. All I have to do is write them next to the corresponding arrow on the exam paper when the time comes.
My client travelled an hour and a half to see me. Her baby is presenting by the breech and therefore she feels that the plan to birth her baby at home will remain just a dream. The grief that women experience when their birth plans are no longer supported by the guidelines isn’t often acknowledged nor appreciated in mainstream maternity care/services. Discarding plans to birth at home is often approached with a sense of pragmatism:
“Sure, it can’t be helped; we just want you and your baby to be safe!”
My fingers palpate the muscles between her shoulder blade and the spine. I haven’t applied the oil yet, I am still finding my bearings. There’s a knot just below the lower third of the right scapula, I explore the consistency of the rest of the muscle and the fibres lead me diagonally towards her lumbar spine. I wonder if this knot can in part be attributed to the stress she’s been experiencing at the prospect of a hospital birth (at best) or (clearly her care providers’ preference) a caesarean section if the baby doesn’t turn.
Almost daily I feel grateful that I had the courage to leave midwifery for good and turn back to full-time body work. There’s nothing like hearing that a mother is finally free from pain or that a baby has turned a few days after a session with me. Helping mothers process their fear of what may lie ahead is part of what I do and it is incredibly rewarding.
Just at the very base of the ribcage I find a piece of the puzzle that will help us unravel the knotted tissue. Then I palpate further down her back and I reach her PSIS, her posterior superior iliac spine. I think that perhaps, by releasing the tight QL muscle I found between her lower ribs and the PSIS, we can bring more balance into the core2 and more space for her baby to move from bum down to head down. We will explore her respiratory diaphragm and abdominal muscles in a little while to see what’s happening between her ribs and hips on the front of her body.
I pour some of her oil blend into my palm, rub my hands together and apply it in long, broad strokes. The scent is released instantly by the heat of her body - Patchouli and Ylang-Ylang. Essential oils have become integral to what I do, my companions in my mission to support, alleviate and release tension.

I look at the image of the pelvic brim beside Sharon and I am trying to fit the eight landmarks on an imagined clock face with the sacral promontory at 12 o’clock and the upper inner border of the symphysis pubis at 6 o’clock. The rest of the landmarks can’t be placed directly on the hour, they are just about a minute out and it’s a shame that there’s one too many. I try it anyway and I put the pubic crest at 5:55 on the left side of the body and at 6:55 on the right. I am initially pleased but then discard the entire idea because I decide that memorising them as a list of eight would likely cause me less confusion in the exam.
As I continue the investigation of my client’s soft tissues I close my eyes and for the first millisecond I see the image of a red line fade into darkness. There are six strands of fine red thread tied around my right wrist. They are fastened together in a small knot that I like to place next to the inside of my wrist, where you apply perfume. I have been wearing them for four weeks already which means that the mama they connect me to is rounder than the last time I saw her, at her blessingway. As the scent of the Frankincense and Ylang-Ylang permeates my little massage space, I think of fascia, my client’s fascia, the incredible crystalloid collagen that provides structure for her body. I think about its responses to the pressure I exert in certain places and its responses to the focus and the intention I communicate to it through my hands, my own fascial network. As soon as I visualise a transfer of energy into her soft tissues, my client’s knot unravels and her muscles spread beneath my touch. “The pain is gone,” she says. We’ve worked together before and she knows what to expect. Her cue lets me know I can move to another area.
I open my eyes and catch sight of the red thread again and it reminds me of what Elly said to Faye, the mama to be, at the blessing as she gave her a print of a pregnant mother surrounded by versions of herself - “You are never alone, we are all connected through time and space. Your sisters and ancestors will be with you at your time of birthing. Remember that.”
A thought forms in my mind: Fascia connects us all - fascia is
our own kind of mycelium.
“Sacral ala, pubic crest, sacral promontory.”
This time Sharon is pointing at the landmarks randomly and she has removed the words from the slide. Today’s lecture is about the foetal skull but the first five minutes are dedicated to making sure we have done our homework.
One trip around the pelvic inlet and we move on.
Sharon is the kind of lecturer who sets boundaries early on in the student-teacher relationship.
Tardiness is not acceptable, nor is chewing gum or talking in class.
I know that doing your homework is an integral part of Sharon’s list of exacting standards that a student midwife should uphold. I respect Sharon more than any of our lecturers and I make sure that I go to her lectures well prepared.
My next client has sore hips.
Sore hips are common in pregnancy and I would say that half of my clients seek me out for help with hip pain.
I ask my usual questions to get an idea as to why she’s so sore.
“Our session today is likely going to help you. For your pain to stay away, we’ll need to look at your postural habits, too.”
She gets up on the couch as I make up her pain relief blend.
I go back to her and I cushion her bump, then her top arm and finally her top leg. Again, I start with exploring the soft tissues around the neck and shoulder blades first.
“Did you know that neck mobility and pelvic mobility are linked?”
Most of my clients are pregnant and I love inspiring them to move in pregnancy for an easier labour. I encourage her to take a deep breath in and exhale slowly and I don’t seek further conversation. If she wants to chat, I am up for it, but I want to give her space to relax into her session.
I get to working on her low back and pelvis. The fascia in her hips release relatively easily.
According to her last midwife appointment, this baby is head down and at 36 weeks I can sense the baby’s vertex - the crown of the head - next to the pelvic brim as I extend my client’s sacrum into a stretch.
She’s in a state of deep rest now.
Good! I know she’ll go back to two young kids, so I love that she is resting.
Through the skin of my hands, through this mother’s skin and bones, through the muscle of her womb, through the amniotic fluid and through the charge that runs through it all. I feel connected, not only to this mama/baby, but to all of creation; such is the power of the fascia.
I take in the image of a baby’s skull Sharon has projected onto the screen at the front of the classroom. She explains that the parietal bones overlap the frontal and occipital bones as the baby moves through the pelvis, a process that starts at the pelvic brim. As the baby enters the pelvic bowl the bones shift further and sometimes, as the baby begins its journey through the pelvic outlet, one of the parietal bones will slide over the other along the sagittal suture line. This temporary overlap of the bones of the foetal skull is called moulding and it is part of the anatomy of childbirth.
We learn the diameters in the various directions through the foetal skull along with the diameters of different levels of the pelvis. The smallest diameters occur when the baby’s chin is tucked all the way down towards his chest. It’s 9.5cm and it is called the Suboccipitobregmatic Diameter - a typical “head down” baby. I am entirely gobsmacked to hear - for the first time - that a baby could also be born face first and that that diameter is also 9.5 cm.
I learn about the obstetric conjugate—the baby's passageway through the pelvis—and that it averages about 10.5 cm in a gynecoid (conventionally female shaped) pelvis - this one can’t be measured, only estimated. I am also introduced to the measurements front to back, side to side, and across the pelvic brim, cavity, and outlet.
The foetal skull will be on the exam paper and so will all of those diameters. This time there’s no pointing and reciting in choir but simply the homework of familiarising ourselves further with the new terminology and to please, please, learn it all off by heart.
As the reality of preparing for this exam hits me, my confidence in memorising those names and numbers begins to wane. There are so many of them!
In the back of my mind a question forms, one that will be gnawing at me for years to come.
Author Bio: Nicole is a former midwife and author of the blog My Journey of Conscious Uncoupling from NHS Midwifery. She practices as a fascia therapist at Essentially Birth, her pregnancy massage clinic in Belfast. Nicole is passionate about the role of the soft tissues in birth and she is the co-creator of the Born Through Yoga Movement for Birth and Nurturing Newborns Programme.
Part two of this reflection will appear in our next publication. Or, to read it in full now, visit Nicole’s blog.
2 Editor’s footnote:The body’s core is the term used for the group of muscles within the abdomen that stabilise the spine and pelvis. QL stands for Quadratus Lumborum.
The AIMS Journal spearheads discussions about change and development in the maternity services.
AIMS Journal articles on the website go back to 1960, offering an important historical record of maternity issues over the past 60 years. Please check the date of the article because the situation that it discusses may have changed since it was published. We are also very aware that the language used in many articles may not be the language that AIMS would use today.
To contact the editors, please email: journal@aims.org.uk
We make the AIMS Journal freely available so that as many people as possible can benefit from the articles. If you found this article interesting please consider supporting us by becoming an AIMS member or making a donation. We are a small charity that accepts no commercial sponsorship, in order to preserve our reputation for providing impartial, evidence-based information.
AIMS supports all maternity service users to navigate the system as it exists, and campaigns for a system which truly meets the needs of all.
{kind=link}