AIMS Journal, 2022, Vol 34, No 2
To read or download this Journal in a magazine format on ISSUU, please click here.

By Alex Smith
In 2011, Vicki Williams asked in the AIMS journal editorial, “Is this label of ‘high risk pregnancy’ doing women any favours, or is it...creating damaging additional stress for childbearing women and those who care for them?”.[1] Eleven years on, with escalating rates of medicalised births and birth trauma, it has become an even more urgent question. Does this label directly or indirectly harm people, and if so, can this be considered as an example of obstetric violence?
It would be wonderful to imagine that women who really do have a higher chance of problems arising during their pregnancy or labour receive particularly gentle and attentive care. Midwife-led care, combined with good inter-professional communication and continuity of carer, improves outcomes,[2] almost certainly because this allows for relationships of trust to develop through which, as deemed essential in the 2020 interim Ockenden report,[3] women and their families are listened to and respected. But all too often, the very things that may have made a positive difference to people labelled as ‘high-risk’ are denied, and thus, the label becomes a self-fulfilling prophecy,[4] a prediction that causes itself to become true.

It may seem strange that two small words, words intended to safeguard, could cause harm. This is how they might:
The emotional resonance of the words: The term ‘high risk’ suggests that danger is ever present. The words alone are enough to fill the labelled person with a constant sense of anxiety, uncertainty and powerlessness. Those feelings, even when very low-key, trigger a rise in the level of the stress hormone cortisol, leaving the person on high alert. At the same time, in a see-saw effect, the hormones that support physiological functioning and well-being are lowered, diverting energy from non-essential functioning and holding it in readiness for coping with the potential emergency. In one (not pregnancy-related) study looking at over 33,000 adults, those who were aware that they had hypertension reported elevated levels of psychological distress compared with those individuals who had hypertension but were unaware of this.[5] While there is a natural rise in cortisol as pregnancy advances, this extra feeling of being ‘at risk’ tips the balance with unfavourable implications for both mother and baby. [6],[7]. Chronic anxiety in pregnancy can increase the chance of hypertension, pre-eclampsia and premature birth;[8] conversely, pregnancy may even become extended, with the body holding onto the baby until the situation feels safer.[9] In labour, if the mother feels ‘at risk’, her body may slow or stall labour to give her time to find a place of safety before the baby is born.[10] Not only is this internalised anxiety upsetting and unpleasant for the mother; there is also growing evidence that even milder forms of maternal stress or anxiety during pregnancy affect the fetus causing possible long-term consequences for infant and child development.[11]
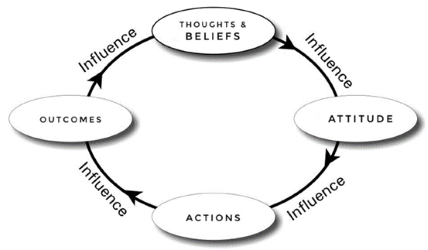
Believing the words: In addition to the effect on hormone levels, the belief that a label of ‘high risk’ means we are in increased danger informs our attitudes and subsequently, our actions.
When people with the label of ‘high risk’ approach the AIMS helpline asking for information about their options, we usually suggest that they ask the labeller (the midwife or doctor) to quantify their chance of the risk manifesting when compared with a person labelled as ‘low risk’. It is usually much smaller than suggested by the label.
Think of two bags of sweets. One (the ‘low risk’ bag A) contains 999 green sweets and 1 red sweet, the other (the ‘high risk’ bag B) contains 998 green sweets and 2 red sweets. It is accurate to say that the chance of selecting a red sweet from bag B is double that of bag A - the risk has risen by 100% - and yet the actual chance of picking a red sweet from bag B is very low indeed, and little different from the chance of picking one from bag A. Of course, all other things being equal, if you definitely want to avoid the risk of a red sweet, bag A is the one to choose, but things aren’t equal. If you know that the bags are handled differently and many more green sweets in bag A will get cracked or crushed compared to the number in bag B, then this may sway your beliefs, attitudes and actions.
Let’s think of this in terms of two women of 40, Rose and Mary, both considering a home or midwife-led unit birth. Rose is told that these options are not advised as she is at ‘high risk’ of stillbirth at her age. That sounds alarming. She believes her midwife (BELIEF), doesn’t feel there is any point in expecting a normal birth (ATTITUDE), and books into the consultant unit (ACTION), immediately doubling her chance of major interventions[13] [14] (OUTCOMES). No one has told her about the risks associated with hospital birth and so she assumes that the complex birth she experiences is a result of her age. Thank goodness she was in hospital. Mary is also told that these options are not advised as she is at ‘high risk’ of stillbirth at her age. That sounds alarming but she can’t quite believe it (BELIEF). Mary has a questioning attitude. She knows that life is not without risk, but she is healthier than many younger women - the word ‘high’ doesn’t ring true (ATTITUDE). She researches the numbers (ACTION) and finds that in 2019 the perinatal death rate for babies of mothers over 40 was about 6.5 in every 1000 births, compared with about 5.2 per 1000 births for those of mothers aged 35 to 39, so that’s an additional 1.3 per 1000 (0.13%). These are figures for the total population and take no account of the fact that the risk for an individual mother is likely to be affected by things like health, lifestyle factors and socio-economic status. Not all people aged over 40 are the same. She also finds that only about 8% of these deaths occur during labour. This means that there is roughly a 0.52 in 1000 chance of her baby dying during the birth compared with 0.42 in 1000 for a younger friend who has been told she is ‘low risk’. Mary empathises with her friend Rose’s decision to have her baby in hospital, but she personally aspires to a birth with minimal intervention and so, on balance, she opts for a homebirth knowing that this is likely to reduce the overall chance of experiencing birth trauma - of being cracked or crushed. That (OUTCOME) matters to her too. Rose’s belief that ‘high risk’ actually means bag B is loaded with the dangerous red sweets, changes the actions taken in a way that increases the chance of a traumatic experience of birth - and the label becomes a self-fulfilling prophecy.
Treating the label: The label of ‘high risk’ also affects the actions taken by the midwife or doctor and is another way that it reinforces the self-fulfilling prophecy. Many doctors and midwives simply believe the label and act accordingly. When asked to quantify the actual risk, and especially the actual risk for a given individual, they will often be stumped. They may not know that it is often very low. Their attitude is likely to be to stick with the protocol as, working within a culture of litigation, this feels safer to them. When women challenge the protocol, the talk about risk will often crank up in a desperate bid to gain the woman’s compliance, and their fear becomes palpable. This is poignantly described by Helen Ward Leese in her personal account of birth. When maternal ‘consent’ is gained by saying to the mother, ‘Do as we say or your baby is in danger’ it is not consent, it is a hostage situation.
Pointing the bone: Considering the harm caused by being labelled ‘high-risk’ put me in mind of the ultimate example of this, the (almost but not quite extinct) Aboriginal practice of Kurdaitcha or pointing the bone.[15] This is a practice whereby an elder or elders from the group sentence someone to death simply by uttering a few words and by pointing a special carved bone in the direction of the victim. The condemned, then free to go but believing the power of the curse with every fibre of their body, dies within days or weeks. It is the deeply embedded cultural belief, in the face of the curse, that changes the person’s physiological functioning and behaviour in a way that ensures it comes true. In Australia ‘to point the bone’ has come to mean: to predict someone's or something's ruin, downfall, or failure, or to cast blame or aspersions on someone.[16] This is exactly what happens when our cultural elders (midwives and doctors that people believe) tell a woman that she is at high-risk of bad things happening because she is too fat or too old or has not gone into labour yet.
So, my plea to midwives, doctors and policy-makers who wish to ‘do no harm’:

The theme of this issue of the AIMS journal is obstetric violence. This is the term used today to describe what happens to people, during their experience of maternity care, that leaves them feeling traumatised - when what happened was avoidable.
We open with an article by Gemma McKenzie who explains the term in greater detail. In particular she shows how much of what women experience as violence is so deeply embedded within the accepted structure of care, that midwives and doctors simply cannot see it at the time - and yet it leaves its scars nevertheless. This is movingly illustrated by Helen Ward Leese’s personal account. It makes for a chilling read but one that could usefully be part of the training of anyone charged with the care of a woman in labour. And moving to much earlier in the conditioning of our cultural attitudes, Beth Whitehead addresses ‘body-shaming’ and the way that this impacts the experience of pregnancy and birth, putting forward a very strong challenge to the use of BMI measurements in decision-making.
Obstetric violence and the law is discussed by legal experts Olivia Verity and Dr Camilla Pickles and midwifery lecturer Leigh Ham write about human rights in maternity care. Echoing Gemma’s reference to the BBC series, ‘This is Going to Hurt’, Heather Spain uses mention of the programme to launch into a passionate analysis of the harms done by the way that the media portrays birth and in particular by the way that the violence is normalised. Kelly Sawyer addresses one such ‘normality’ - the routine or even mandatory vaginal examination, that many women feel they have no choice but to accept. Kelly describes how her NHS Trust is running the Respectful Vaginal Examinations Project to improve practice and educate pregnant people about their rights; while activist Mara Ricoy tells the AIMS campaigns team about her inspiring international movement to tackle obstetric violence: The Roses Revolution.
The idea of normalised violence within maternity care is not a new one. Midwifery student Antonita Kirubanathan reflects on Frédérick Leboyer’s 1974 still-revolutionary book Birth Without Violence, with his emphasis on the baby’s experience. UK Resuscitation Council Newborn Life Support Instructor, Joanne Foster, talks about newborn life support, and how today this reflects a stronger and gentler understanding of the newborn’s transition to life outside of the womb. The themed articles for this issue also include a very hopeful account, from Julia Adams and Pat Ballantyne, of the evidence for Emotional Freedom Technique ‘tapping’ (EFT) as a fast, gentle and successful treatment for those people who have been left feeling traumatised by their maternity care experience.
Moving on from the themed content, we have three book reviews: Anne Glover looks at Sallyanne Beresford’s interesting and informative book ’Labour of Love’, aimed at birth partners; Keren Williams reviews Laura Godfrey-Isaacs and Samantha McGowan’s interactive book ‘Maternal Journal: A creative guide to journaling through pregnancy, birth and beyond’; and Sue Boughton reviews Penny Simpkin’s ‘The Birth Partner’ and concludes that it is a book justifiably on its 5th edition.
Following the recent Ockenden Report, Cyril Chantler - deputy chair of NHS-England’s Maternity Transformation Programme’s Stakeholder Council - offers his immediate reflections highlighting the broader context of ongoing maternity transformation in England. Continuing to push for continuity of carer, AIMS Volunteer Georgia Clancy reports on researchers at King's College London who have been exploring the implementation of continuity since the Better Births report. In one article, The AIMS Campaigns Team give us an insight into their priorities for 2022-2023; in another they summarise why continuity of carer is so important and how team members have been working with others to support its implementation.; and in a third they introduce their new series of position papers explaining why they have produced them and how they hope they will be of use. Last but not least, The AIMS Campaigns Team let us know what they have been writing, reading, viewing and doing in their vital work.
[1] Williams V. (2011) Is the ‘high risk’ label helpful? www.aims.org.uk/journal/index/23/4
[2] Sandall, J., Soltani, H., Gates, S., Shennan, A. & Devane, D. (2016) Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database of Systematic Reviews. (4). Available from: https://doi.org/10.1002/14651858.CD004667.pub5
[3] Ockenden Report (2020) page 27 www.ockendenmaternityreview.org.uk/wp-content/uploads/2020/12/ockenden-report.pdf
[4] Schaedig D. (2020) Self-Fulfilling Prophecy and The Pygmalion Effect www.simplypsychology.org/self-fulfilling-prophecy.html
[5] Hamer M, Batty GD, Stamatakis E, Kivimaki M. Hypertension awareness and psychological distress. Hypertension. 2010 Sep; 56(3):547-50. https://pubmed.ncbi.nlm.nih.gov/20625078
[6] Lilliecreutz, C., Larén, J., Sydsjö, G. et al. Effect of maternal stress during pregnancy on the risk for preterm birth. BMC Pregnancy Childbirth 16, 5 (2016). https://doi.org/10.1186/s12884-015-0775-x
[7] Centre for Cardiovascular Science (2020) Stress during pregnancy may change brain development in babies. www.ed.ac.uk/cardiovascular-science/news-events/news/stress-pregnancy-baby-brain-development
[8] Vianna P, Bauer M E, Dornfeld D, Chies J A B, (2011) Distress conditions during pregnancy may lead to pre-eclampsia by increasing cortisol levels and altering lymphocyte sensitivity to glucocorticoids. Medical Hypotheses. Volume 77, Issue 2,Pages 188-191,ISSN 0306-9877, https://doi.org/10.1016/j.mehy.2011.04.007. (www.sciencedirect.com/science/article/pii/S0306987711001708)
[9] Margerison-Zilko et al. (2015) Post-term birth as a response to environmental stress: The case of September 11, 2001 https://academic.oup.com/emph/article/2015/1/13/1795340?login=false
[10] Lothian J. A. (2004). Do not disturb: the importance of privacy in labor. The Journal of perinatal education, 13(3), 4–6. https://doi.org/10.1624/105812404X1707
[11] Zietlow A. et al (2019) Emotional Stress During Pregnancy – Associations With Maternal Anxiety Disorders, Infant Cortisol Reactivity, and Mother–Child Interaction at Pre-school Age. www.frontiersin.org/articles/10.3389/fpsyg.2019.02179/full
[12] Back in shape clinic (2021) Pain, Prophecy and Placebo: How the way you think can change the way you feel. www.backinshape.co.uk/pain-prophecy-and-placebo
[13] The Conversation (2019) Having a baby at a birth centre is as safe as hospital but results in less intervention https://theconversation.com/having-a-baby-at-a-birth-centre-is-as-safe-as-hospital-but-results-in-less-intervention-125732
[14] Statistician Marjorie Tew analysed the results of the British births 1970 survey and found that then and in the preceding decades, births in all risk groups were safer taking place at home or in a GP unit. That is not to say that poor outcomes did not increase in each risk group, but they increased even more when the birth was in hospital. As research into safety and place of birth is confined to ‘low-risk’ groups today, we have no idea if this may still be true.
Tew M. (1985). Place of birth and perinatal mortality. The Journal of the Royal College of General Practitioners, 35(277), 390–394.
[15] Lipke I (2014) Curses and Cures: Superstitions http://unusualhistoricals.blogspot.com/2014/11/curses-and-cures-superstitions.html
[16] Dictionary definition - https://idioms.thefreedictionary.com/point+the+bone+at
[17] Dagustun J (2012) Beware the Dead Baby Card. www.aims.org.uk/journal/item/beware-the-dead-baby-card
The AIMS Journal spearheads discussions about change and development in the maternity services.
AIMS Journal articles on the website go back to 1960, offering an important historical record of maternity issues over the past 60 years. Please check the date of the article because the situation that it discusses may have changed since it was published. We are also very aware that the language used in many articles may not be the language that AIMS would use today.
To contact the editors, please email: journal@aims.org.uk
We make the AIMS Journal freely available so that as many people as possible can benefit from the articles. If you found this article interesting please consider supporting us by becoming an AIMS member or making a donation. We are a small charity that accepts no commercial sponsorship, in order to preserve our reputation for providing impartial, evidence-based information.
AIMS supports all maternity service users to navigate the system as it exists, and campaigns for a system which truly meets the needs of all.
 [12]
[12]