AIMS Journal, 2026, Vol 38, No 1
By Alex Smith
Throughout history people have seen education as having different purposes. Or, to put it
another way, there are a number of different philosophies of education, and this applies
equally to childbirth and parent education.1
As a parent, Mildred feels it is important to enquire about the aims of an antenatal course to ensure that she knows what she is getting for her money. If she was going to spend £200 to £300 or more on a flashy gizmo being sold to expectant parents she would naturally ask: what is it for (what is the point of it)?; will we actually use it?; and if we do, will it make a positive difference in our lives? She intends to ask the very same questions before she decides on an antenatal course. This is what she discovers:
Mildred discovers that many antenatal education providers, even charitable ones, run their service like a business. The course therefore needs to be attractive to potential parent ‘customers’. However, not all parents share the same values and aspirations so, in order to expand the business (reach as many ‘customers’ as possible) and remain financially viable, the course content needs to be watered-down to create an economical, one-size-fits all product that can be delivered in the least time possible with the highest possible rate of customer satisfaction - with satisfaction being evaluated at the end of the course but before the birth - that is, before the product has been put into use. The approach is called TQM or Total Quality Management. Quality is a fine word - but what is quality in the context of antenatal education; quality of what?
To answer that question we can borrow Kirkpatrick’s model of evaluation. This model is intended to measure workplace training courses, but it can be applied to measuring the usefulness of a course of antenatal education. It has four levels:
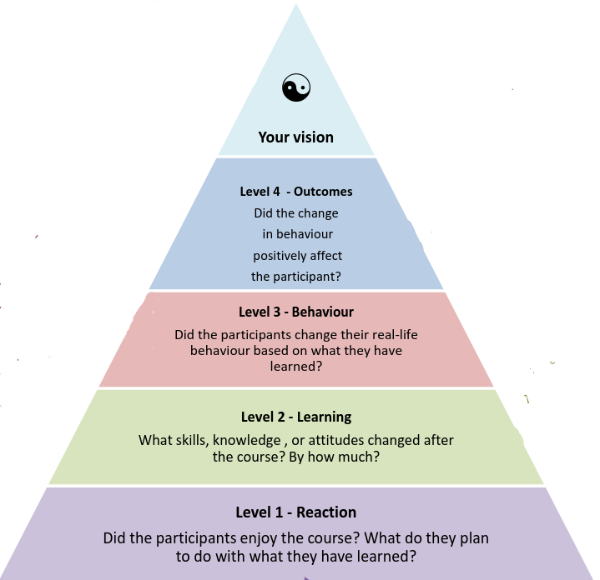
Was the course engaging and did it feel relevant to most parents? - Evaluated by positive post-course feedback before the birth.
Did parents develop knowledge, skills and confidence? - Evaluated through course activities that put learning to the test.
Did parents put learning into practice in real life situations? - Evaluated after the birth by listening to parent reports.
When parents put learning into practice, did this make a positive difference? - Evaluated by listening to parent reports.
There is a peak (a point) to the 4 levels. It is not a fifth level but ‘an intention’ for what the educational provider hopes she might see over time if a course is evaluated well at all four levels. For example, she might notice that women who attend the course: are more likely to have a positive experience of birth; continue breastfeeding for as long as they had hoped; or report lower levels of postnatal unhappiness.
Unfortunately, some providers are only concerned with level one, and, at a push, level 2. When asked by Mildred, they may not be able to say what the point (or aim) of their course is - what positive difference they would hope to see if parents actually used their new learning. They may look rather blankly at her as if that is a stupid question - but, as a paying parent, Mildred wonders whether a course where she learned things that she was unable to use, and where it didn’t really seem to help in real life, is a quality course - even if it was fun at the time and she made some nice friends. Does such a course count as education or is it simply an antenatal briefing and a social opportunity?
This is why true educators will also evaluate at levels 3 and 4, and that can only happen after the baby is born. They will be keen to create a relaxed setting for a course reunion where parents feel safe enough to talk openly about their experiences with people they have come to know and trust, and where they feel truly heard. Only then will they be able to gauge whether the learning was educational in any meaningful way - meaningful depending on the individual parent’s and the individual provider’s philosophy of education and whether these were happily aligned or not.
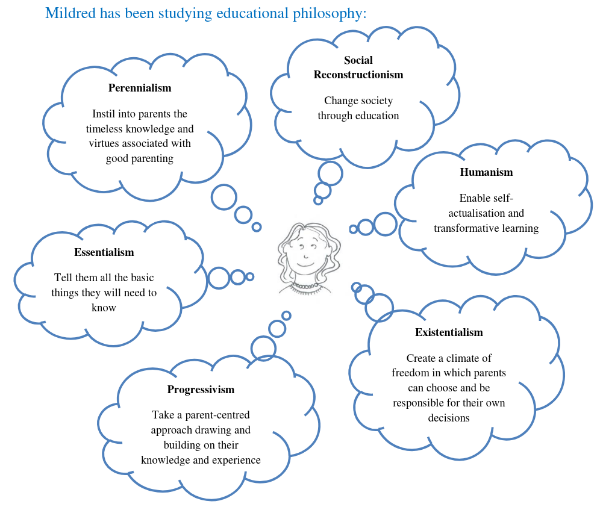
 Mildred takes a look at some different philosophies as they may apply to antenatal education to consider which ones resonate most with her own.
Mildred takes a look at some different philosophies as they may apply to antenatal education to consider which ones resonate most with her own.
Perennialism: Perennialism in antenatal education focuses on the timeless, fundamental truths about the human experience of birth and parenting. It emphasises enduring principles that have remained relevant for generations. These may include: the experience of physiological birth; the need for resilience; living with uncertainty; the value of family and cultural traditions and rituals; parenting around the clock; and understanding the universally shared emotions encountered by parents from the dawn of time. The educator may be viewed as an ‘expert guide’ (an older ‘sister’) sharing woman-to-woman wisdom, not imposing her own ideas but using Socratic methods to encourage critical thinking. Critical thinking allows parents to disentangle their inherent strengths and native instincts from the confusion of modern and ever-changing cultural constructs, and, in the process, to develop a sense of ‘affinity with the elders’ that holds them through a smoother and more confident transition into parenthood - which is the teacher’s aim.
Social reconstructionism: Social reconstructionism in antenatal education aims to ‘change the world’ by educating parents to be the agents of change. This is teaching people to ‘be the change they want to see in the world’. The course would foster critical consciousness about the politics of birth, with parents feeling like active participants in a movement to create a better birth world. The approach encourages women and partners to recognise and question power relationships within the system, to know about women’s legal and human rights and how to take ownership of their birthing and parenting journey. The aim would be to see a larger proportion of women (empowered by the way that course-learning equipped them) navigating the system on their terms, with a good number of those women inspired to help change the system for their sisters, daughters and granddaughters. An example of this approach was seen in the ‘Our Bodies Ourselves’ movement that started in the US in the 70s and continues today.
Humanism: Humanism in antenatal education offers a person-centred, relational, and holistic approach that focuses on the psychological, emotional, and physiological well-being of the woman, valuing her autonomy, dignity, and capacity to give birth - trusting that each woman knows what is best for her and what she needs. The course will focus on informed decision-making and will hold physiological birth (how humans give birth) as a neutral, healthy reference point in the discussions. By contrast to the current ‘technocratic’ model of birth that separates mind from body and views the body as a machine, a humanist approach stresses mind-body integration and views the body as an organism that requires certain conditions in order for it to flourish. The humanist course of antenatal education explores these things with the parents in a way that respects their diversity and individuality and helps them to prepare for a sense of coming into their full selves (transformative learning or ‘self-actualisation’) - which is the teacher’s aim.
Existentialism: Existentialism in antenatal education considers the birth of a child not merely as a physiological event, but as a profound, life-altering experience that triggers existential reflections, including questions about meaning in life, mortality, freedom, isolation and responsibility. It incorporates holistic, philosophical, and spiritual dimensions, encouraging parents to explore their own values and be better able to cope with the ‘existential vulnerability’ of becoming parents, resulting in improved postnatal mental health, which is the aim of the teacher. Parents explore the transition into parenthood as a metamorphosis involving a loss of a former identity and the development of a new one - (read Matrescence,) The focus is less on a particular topic, and more on what that topic means for the individual. For example, ‘what would having a caesarean mean for you?’, or, ‘what does it mean to be a father?’. Meaningfulness is a core component of the concept of ‘sense of coherence’ (SOC), and SOC is a central concept in the salutogenic approach, and so salutogenesis (a focus on what causes good health) is central to an existentialist antenatal course. Working through the medium of the body would be a natural part of a salutogenic approach, and, as the mystery and meaning of life transitions are more easily explored through the arts, techniques like storytelling, birth art, poetry, and the use of metaphor such as the labyrinth would feature strongly.
Progressivism: Progressivism in antenatal education places a strong emphasis on the use of human experience as the basis for knowledge, shifting the focus from the simple transmission of information to the drawing out and development of the parents’ existing knowledge and experience. Progressivism reflects a belief in the importance of experiential learning, collaborative learning, critical thinking, and problem-solving and the teacher uses methods such as small-group work using case scenarios, role play, group discussion, and the practice of physical skills. Parents may even be asked to research topics and share their knowledge with the group. The aim is that parents will be thinking and advocating for themselves, making their own decisions, and, having assembled the required resources, taking responsibility for themselves and their babies as part of a supportive community.
She would emerge:
Feeling a sense of ‘affinity with the elders’ that holds her through a smoother and more confident transition into parenthood. The words ‘rooted’ and ‘grounded’ come to mind.
Empowered and equipped to navigate the system on her terms and able to pass the skills of self-efficacy to others. The term ‘being a holder of authoritative knowledge’ comes to mind.
Transformed or metamorphosed into the stronger, fuller person she wants and needs to be as a mother. The word ‘matrescent’ comes to mind.
Better able to cope with the inevitable existential vulnerability of parenthood and enjoy improved mental well-being as a result. The word ‘resilient’ comes to mind.
Thinking, advocating and taking responsibility for herself and her baby as part of the supportive community she has helped create. The words ‘autonomous'. ‘exercising self-efficacy’ and 'connected' come to mind.
Wow, she thinks, there really is a point in attending that course. £200-£300 would be cheap at the price!
Such an education would ideally begin early in pregnancy, ‘walking with’ Mildred as she makes the biggest transition of her life. It would allow for new ideas to be slowly and gently assimilated over time and for practical and physical skills to be developed and practiced again and again. The skills of decision-making, advocacy and assertiveness would be rehearsed until they felt like second nature. The layered learning approach, along with emotional engagement with the ideas (through the use of story, art, physicality and discussion) would mean that learning is gradually internalised - taken into the affective learning domain, strengthening values, beliefs and motivations, and hence, informing the actions Mildred is able to take to safeguard herself. That course would really make a difference. It would be an education for life.
This rich and transformative course would really make a difference but it would require time and commitment. It could be structured like a long and flowing ‘stream’ running throughout the course of pregnancy and beyond - or - like a more contained, warm, safe and private ‘pool’ in which to relax and exchange wisdom, knowledge and skills during the final months of pregnancy.
The ‘long and flowing stream’ course would welcome women at all stages of pregnancy and early motherhood, first timers and experienced mothers, with the former learning from the latter, and the latter learning from their chance to be heard. Some sessions might include partners and some might be just for the women. As with a river, the same ground would be covered repeatedly but often in a different light and there would always be something new to consider. It would be a moving, responsive and organic course with time to safely flow into the dark depths of life and then even more time to wallow in the warm shallows and share tea and cake together. This is the course that Mildred hopes to find.
The ‘warm contained pool course’ could be offered in the third trimester for small intimate groups of up to 12 people, and with closed membership. This would offer a fluid and personalised curriculum with room for movement (of content and well as for the practice of physical skills) and with plenty of time for relaxation and reflection.
What Mildred actually finds - the course that is most prevalent in antenatal education today - is the compact, ‘urban block, one-size-fits-all course’. She finds it has gone all out to adopt an Essentialism philosophy.
Essentialism: Essentialism in antenatal education offers a compact and standardised briefing on current, mainstream information about birth and early parenting - just the essentials. There is a place for basic information, but on its own, it does not constitute education.
The ‘urban block, one-size-fits-all course’ may (or may not) pay lip-service to informed decision-making and physical skills for birth, but, at best, this would be brief and in passing, with no time for consolidated and repeated practice. There may well be small slots for one-off topic-based discussions and activities, but the pre-set curriculum will be tightly packed with basic information about ‘what to expect,’ so there will be little or no time for deeper discussions about what this information means for individual parents - certainly not for discussion that builds week by week as ideas (and their potential implications) start to sink in. Similarly, there will be little or no time for exploring the politics of birth, the power hierarchies within the maternity care system, how to navigate the maternity care system on your own terms - and why you may have wished you had - and certainly no time for considering the meaning of life or for trying out birth art.
The essentialist approach relieves parents from ‘uncomfortable learning’ - the sort that may sometimes elicit accusations of bias, but also the sort that may have made a difference - and hence it perpetuates the status quo. Content, teaching methods and teaching aids (including online resources, powerpoints and so on) are standardised with the idea of looking ‘professional’ but, in the process, diminishing the individual educator’s creativity, authenticity and passion. The essentialist course could fairly easily be replaced by a few leaflets and a coffee morning, so the provider may reasonably think that highly trained and motivated educators are not required anyway. The aim is to hand over the same neatly packaged bundle of basic information (to as many customers as possible) with no clear intention that this will make a positive difference for anyone.
Mildred wonders what the point of such a course is. It may pass the time, get her out, help her make some new friends (all fine in themselves - it may even be fun) - but she, and many like her want and need much more than this from a course of education - especially given the current birth climate of fear, trauma and over medicalisation. However, many parents have not studied educational philosophy or the politics of birth as Mildred has. First time parents, in particular, may be very attracted by the marketing for the neatly bundled, essentialist ‘gizmo’ course without even wondering what the point of it is or whether it even works.
Mildred’s message to these parents is:
Author Bio: Alex is the editor for the AIMS journal, a grandmother and great grandmother, and witness to some truly wonderful physiological births. She has close to half a century’s experience as a childbirth educator.
1 Wilkerson NN. Perspectives on learning for childbirth educators. J Perinat Educ. 2000 Summer;9(3):11-8. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1595026/
The AIMS Journal spearheads discussions about change and development in the maternity services.
AIMS Journal articles on the website go back to 1960, offering an important historical record of maternity issues over the past 60 years. Please check the date of the article because the situation that it discusses may have changed since it was published. We are also very aware that the language used in many articles may not be the language that AIMS would use today.
To contact the editors, please email: journal@aims.org.uk
We make the AIMS Journal freely available so that as many people as possible can benefit from the articles. If you found this article interesting please consider supporting us by becoming an AIMS member or making a donation. We are a small charity that accepts no commercial sponsorship, in order to preserve our reputation for providing impartial, evidence-based information.
AIMS supports all maternity service users to navigate the system as it exists, and campaigns for a system which truly meets the needs of all.